Intelligence on remote surgical collaboration, telepresence, and the future of the operating room.
Topics: remote surgical training · surgical telepresence · MedTech innovation · AI in healthcare · telementoring · case support
When was the last time your best surgeon had to get on a plane to support a case?

From telementoring to telesurgery: understanding the spectrum
Remote surgical training has crossed from experimental to established.
That isn’t a marketing claim. A February 2026 systematic review in BMC Medical Education examined 27 studies — including 15 randomized controlled trials — and found that synchronous remote teaching achieves training outcomes equivalent to traditional in-person instruction.
A few months earlier, a global Delphi consensus of 23 international experts affirmed telementoring as essential infrastructure for the surgical AI era — not an interim measure.
Together these two papers mark a shift. The evidence base is no longer thin. The field is no longer waiting on it.
Remote surgical collaboration isn’t one thing. It’s a continuum.
At one end is telementoring — an experienced surgeon guiding a colleague performing the procedure on-site in real time. No robotic system required. No infrastructure beyond a surgical-grade connection. Just the right expert, present in real time, in a room they are not physically in.
At the other end is full telesurgery — a surgeon controlling robotic instruments to operate on a patient thousands of kilometers away. Technically demanding, infrastructure-intensive, still emerging as a clinical standard.
The relationship between these two isn’t competition. It’s evolution.
Telementoring is the foundation. Telesurgery is the projected future. The organizations building fluency in remote surgical collaboration today are the ones best positioned to move along that spectrum as the field matures.
The systematic review also confirmed something quieter but consequential: live remote teaching outperforms self-directed video content. The medium doesn’t drive learning. The live expert connection does.
In 2025, two consensus papers (World Journal of Surgery, 2025) — authored by groups including clinical leaders and consultants from Medtronic, Johnson & Johnson, and Intuitive Surgical — defined the roadmap. Five operating models for remote surgery. The majority of them deliverable are today, without robotic infrastructure.
The roadmap has been written. The foundation is telementoring. The destination is telesurgery. The infrastructure connecting the two already exists.
What this means in practice
The Greenland case makes it concrete.
In 2025, Rigshospitalet in Copenhagen connected to Nuuk across 3,500 km — because Greenland has no resident neurosurgeon. Patients previously faced either medical repatriation to Denmark or no intervention at all. Consecutive cases were completed successfully using remote expert guidance. The programme is now embedded in the standard of care, with extension to the Faroe Islands underway. (BMJ Global Health, 2025.)
That isn’t a pilot. That’s a structural shift.
Dr Alex Nap, Interventional Cardiologist at Amsterdam UMC, described what this looks like from inside a clinical team. His fellows perform procedures in the cath lab. When they have a question, he used to walk through the entire hospital to answer it. The problem was never expertise — it was the delay in accessing it.
With cORe One Touch, that delay is gone. One-button press from cath lab to expert — colleague-in-the-room presence on demand.

The 5 operating models — and where Rods&Cones plays
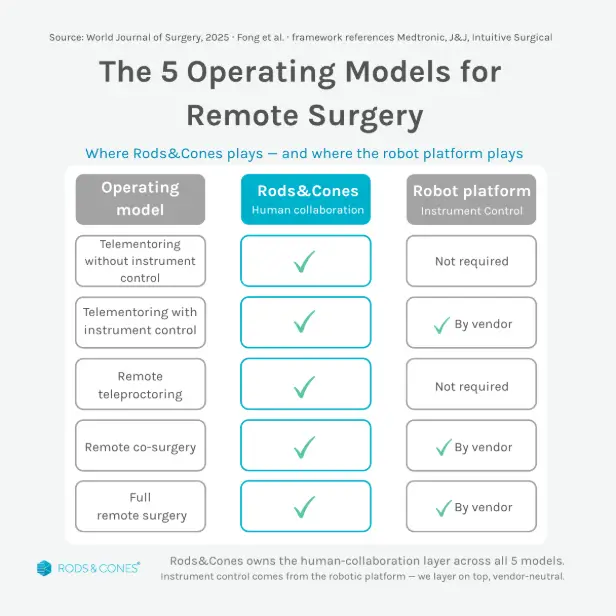
The 2025 consensus framework (World Journal of Surgery, 2025) defines five operating models for remote surgery — from telementoring without instrument control through to full remote surgery. Rods&Cones delivers the human-collaboration layer across all five.
Where instrument control is required, we layer on top of the robotic platform — vendor-neutral, complementary, never competing with the console. You don’t need a robot installed to get value from remote surgical collaboration. You need the right expert in the room. Now.
Going deeper
The five-model framework defines the future. In practice, the learning journey starts one step earlier.
Before a surgeon is guided through a procedure, they need to have seen it. Not an edited highlight reel — the complete, unedited reality of a live case. The decisions. The complications. The moments that never make it into a training video.
Before telementoring, there’s observation. Live surgical streaming is where the journey starts — and the same infrastructure carries it all the way to telesurgery.
The full continuum: observe → learn → be assessed → collaborate.
So, when was the last time your best surgeon had to get on a plane to support a case?
They don’t have to. They have to be one button press away.
For the complete evidence base, we’ve published the full industry report: The State of Remote Surgical Training 2026.